Marketing
Med Spa Cost Per Lead: Why a Lower CPL Can Cost You Money
Your agency cut CPL from $95 to $42 and revenue dropped. Here's why cost per lead misleads med spa owners, and the metric that actually predicts profit.


Your agency sends the monthly report. Subject line: good news.
"We cut your cost per lead from $95 to $42."
That's a 56% improvement. The chart shows a big green arrow pointing down. Everything looks like progress.
The front desk says the leads were flaky. The agency says the campaign improved. The EMR says revenue was flat. Three parties, three different truths — all of them technically correct.
But here's what the report didn't tell you:
83 leads came in. 14 booked an appointment. 9 actually showed up. 5 no-shows — roughly $2,500 in lost revenue from appointments that were scheduled but never happened.
CPL down 56%. Revenue down 26%. The report looked better. The business got worse.
This is the danger of optimizing for cheap leads: when CPL becomes the primary success metric, the system gets optimized to produce it — often at the direct expense of lead quality. More leads, cheaper leads, worse patients.
This article explains why CPL became the standard, why optimizing for it can actively damage your funnel, and what to measure instead.
Why CPL Became the Default Metric
Cost per lead didn't become the standard reporting metric because it's the most useful. It became the standard because it's the easiest to measure.
Ad platforms — Meta, Google — generate leads. They can track form submissions, phone calls, website conversions. That data is available in the dashboard, calculated automatically, updated in real time. An agency can pull it in seconds and put it in a report.
What happens after the lead submits — whether they book, show up, purchase — lives in your scheduling system, your CRM, your EMR. The agency doesn't have access to those. Even if they did, connecting ad-level data to EMR-level revenue requires integration work that most med spa setups don't support automatically.
So the reporting defaults to what's available: impressions, clicks, CPL.
CPL is useful for diagnosing top-of-funnel efficiency. For comparing two similar campaigns with similar offers and audiences, it's a reasonable relative signal. It becomes dangerous when it becomes the success metric — because that's when agencies start optimizing for it directly.
There's also an incentive problem. Agencies are evaluated on the metrics they report. CPL is a metric agencies can directly influence by adjusting targeting, bidding, and offer type. Cutting CPL from $95 to $42 looks like a clear win in a monthly report. Whether that improvement actually translated to more revenue is a harder question — and one that requires data the agency doesn't have.
This doesn't mean agencies are being dishonest. It means the reporting structure has a built-in blind spot at exactly the moment that matters most: after the lead arrives.
The Math Behind "Good CPL"
Here's what happens when you follow the CPL number all the way through to collected revenue.
Scenario: CPL improves from $95 to $42
Previous month (CPL $95):
Ad spend: $4,750
Leads: 50
Booked: 22 (44%)
Showed: 18 (82%)
Treated: 14 (78%)
Average ticket: $650
Revenue: $9,100
Cost per paying patient: $339
This month (CPL $42):
Ad spend: $4,750
Leads: 113
Booked: 32 (28%)
Showed: 21 (66%)
Treated: 14 (67%)
Average ticket: $480
Revenue: $6,720
Cost per paying patient: $339
Same spend. Same cost per paying patient. But revenue dropped by $2,380 — because the cheaper leads were lower quality. Lower booking rate, lower show rate, lower average ticket.
The acquisition cost didn't improve. The patient value got worse.
CPL improved by 56%. Revenue declined by 26%. ROI got worse while the report looked better.
This is what CPL optimization often produces: a funnel that generates more activity at the top while quietly degrading quality below. And because cost per paying patient was the same, even that metric didn't catch it. To see the full picture, you need revenue per campaign — not just cost per patient.
This pattern is common when agencies optimize for lead volume: they broaden targeting, use lower-friction offers, reduce qualifying questions — all of which generate more submissions at lower cost while downstream quality deteriorates. The problem isn't visible until you connect CPL data to booking, show, and revenue data. Which most clinics never do.
Three Ways CPL Misleads You
1. Cheaper leads are often lower quality
The fastest way to reduce CPL is to lower friction: broader targeting, softer offers, cheaper promos, instant lead forms, fewer qualifying questions. That creates more leads — but often fewer patients.
Lower CPL often comes from attracting people who are easier to reach, not people who are more likely to buy. Wider targeting, looser interest parameters, low-commitment offer types — all of these generate more submissions at lower cost. They also tend to generate leads with lower intent who are less likely to book, show up, and purchase.
A $42 lead who never books is worth $0. A $95 lead who books a $1,200 filler treatment and returns twice a year is worth several thousand dollars. CPL cannot tell you which one you have.
2. Not all leads are the same — and CPL treats them identically
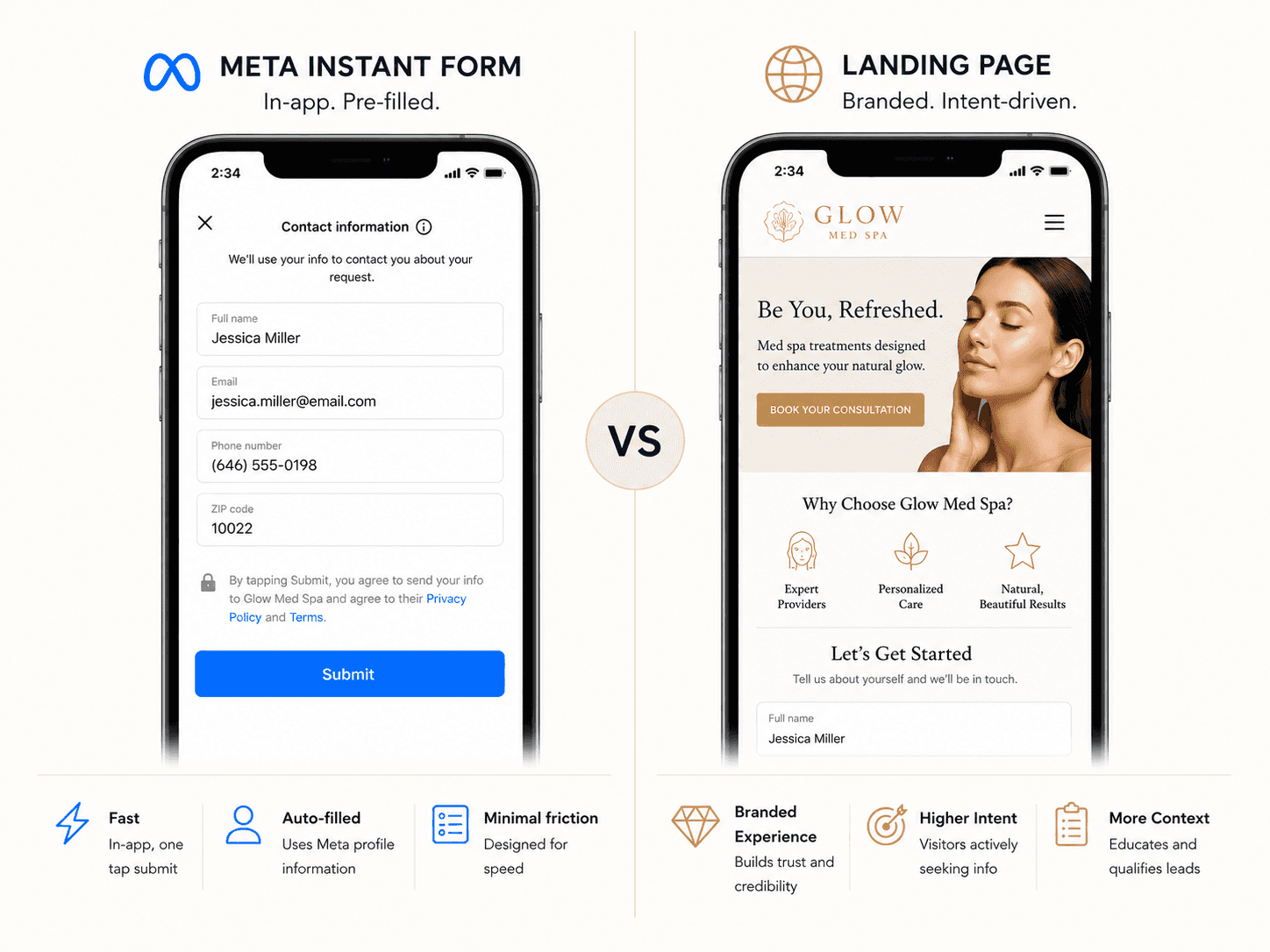
"Lead" sounds like one thing. In practice, it covers very different levels of intent:
Lead type | Typical intent level |
|---|---|
Meta instant form | Low friction, often lower intent |
Website form submission | Medium intent |
Phone call inquiry | Higher intent |
Google search inquiry | Usually higher immediate intent |
Booked consultation | Strongest intent |
A Meta instant form lead — where someone taps "Get Info" without leaving the app — is structurally different from someone who searched "Botox near me," visited your site, read your reviews, and filled out a contact form. Both count as one "lead" in the CPL calculation. The difference in downstream quality can be significant.
Service mix makes this worse. A $42 lead for a $150 facial promotion is not the same as a $95 lead for a $1,200 filler treatment. When CPL averages across different offers and intent levels, the number becomes almost meaningless as a quality indicator.
3. CPL doesn't account for no-shows
No-shows are one of the most expensive inefficiencies in med spa operations. A no-show represents full ad spend to generate a lead, full follow-up effort to convert the lead to a booking, and a reserved appointment slot that produces zero revenue.
In many clinics, no-show rates vary significantly by campaign. A campaign that generates cheap leads from a low-commitment offer may produce consistently higher no-show rates than a campaign with higher CPL but more intent-driven audience. CPL averaging hides this variation entirely.
4. CPL ignores average ticket, patient quality, and lifetime value
Not all patients are equal. A campaign that fills your calendar with patients booking $150 introductory facials is structurally different from one that attracts patients purchasing $900 filler treatments — even if both campaigns show the same CPL.
The revenue per patient matters. The likelihood of that patient returning matters. The treatment mix matters. None of this is captured by CPL.
The best campaign may not have the lowest CPL or even the lowest cost per paying patient on first visit. It may be the one that produces patients who return every 3–4 months for repeat Botox, enroll in memberships, or refer others. In injectables especially, the revenue difference between a one-time patient and a loyal returner compounds significantly over 12 months. First-visit CPL tells you nothing about which type of patient a campaign is attracting.
What to Track Instead: Cost Per Paying Patient
The metric that answers the question CPL can't is cost per paying patient — sometimes called cost per acquired patient or true CPA.
Formula: Ad spend ÷ Number of patients who received and paid for treatment = Cost per paying patient
This number accounts for everything CPL ignores: the leads who never booked, the bookings who never showed, the consultations that didn't convert. It gives you the actual cost of acquiring one revenue-generating patient from a specific campaign.
For a more complete picture, track these four metrics together:
1. Booking rate — what percentage of leads actually scheduled an appointment. Tells you about lead quality and follow-up effectiveness.
2. Show rate — what percentage of booked appointments resulted in a visit. Tells you about commitment level and confirmation workflow quality. Varies significantly by campaign in most clinics.
3. Cost per paying patient — total ad spend divided by patients who received treatment. The clearest measure of campaign efficiency.
4. Revenue per campaign — total collected revenue traceable to a specific campaign. The only metric that tells you whether a campaign made money.
These four numbers together paint a complete picture. CPL alone paints a quarter of it — the quarter that happens to be most favorable to the agency.
Why Your Agency Reports CPL and Not This
When you ask an agency why they don't report cost per paying patient or revenue per campaign, the honest answer is usually one of two things.
"We don't have access to that data." This is often true. Your EMR revenue data lives in your systems, not theirs. Connecting ad spend to collected revenue requires integration between your ad platforms, booking system, and EMR — plumbing that most clinics haven't built.
"We can't control what happens after the lead." Also true. Booking rate depends on your follow-up speed. Show rate depends on your confirmation workflow. Consultation conversion depends on your front desk and injector. An agency can drive qualified leads and still see poor downstream metrics because of operational issues inside the clinic.
Both points are valid. They explain the gap without excusing it.
The problem is when the conversation stops at CPL because it's convenient — not because it's sufficient. An agency that genuinely wants to prove ROI should want to see downstream data, even if they can't control it. The ones who push back on expanding the metrics conversation are usually the ones whose results look worse when you look further down the funnel.
A Better Conversation to Have With Your Agency
You don't need to replace your agency to get better visibility. You need to change what you ask for.
Here's a simple framework for a more productive monthly conversation:
Ask for the funnel breakdown, not just leads: "Of the leads generated last month, how many booked an appointment? How many showed up?"
If they can answer this — because they're tracking through to your booking system — you have a more transparent agency than most. If they can't, that gap is the problem to solve.
Ask about show rate by campaign: "Which campaigns are producing the highest show rates? Which are lowest?"
This tells you something CPL never does: whether the people clicking your ads are genuinely interested or just responding to a low-commitment offer.
Share your revenue data: "Here's what we collected this month from new patients. Can we try to connect this back to which campaigns drove those visits?"
Even a rough reconciliation — matching new patient names to lead sources — gives you directional signal that CPL alone cannot. It's imperfect, but it moves the conversation from activity metrics to business outcomes.
The CAC Calculation Most Clinics Get Wrong
There's a specific math error that affects almost every clinic evaluating marketing performance: underestimating true customer acquisition cost (CAC) because they're using CPL as a proxy.
Here's how the error compounds:
CPL: $55
Booking rate: 35% → cost per booked appointment: $157
Show rate: 70% → cost per visit: $224
Treatment conversion: 70% → cost per paying patient: $320
The owner thinks their acquisition cost is $55 because that's what the agency reports. The actual cost per paying patient is $320 — nearly 6x higher.
This matters for every business decision that depends on CAC: how much to spend on ads, whether to increase budget, how to evaluate a new campaign, whether a service is worth promoting. Decisions made on CPL produce systematically overoptimistic math.
If you've never done this calculation for your own campaigns, it's the most valuable fifteen minutes you can spend on marketing this month.
Quick CPL Audit: Five Questions to Ask This Month
You don't need new software to start seeing through CPL. These five questions will tell you quickly whether your CPL improvement is real or cosmetic.
1. Which campaign had the lowest CPL last month? Identify it specifically — not overall, but by campaign.
2. How many of those leads actually booked? Calculate booking rate for that campaign specifically. If it's materially lower than your other campaigns, the cheap leads aren't converting.
3. How many showed up? Show rate by campaign. A low-CPL campaign with a 40% show rate is performing worse than a high-CPL campaign with an 85% show rate.
4. How much revenue came from those patients? This requires connecting your booking data to your EMR. Even a rough manual reconciliation — matching patient names from that campaign to revenue records — gives you directional signal.
5. What was the average ticket? Were these patients booking $150 introductory offers or $900 treatments? The answer changes the economics entirely.
If you can answer all five, you have enough to evaluate whether your CPL improvement translated to actual business results. If you can't answer most of them, that gap is the real problem.
The Bottom Line
CPL is not a useless metric. It tells you something about ad efficiency at the top of the funnel — and for comparing similar campaigns with similar audiences, it's a reasonable relative signal.
What it cannot do is tell you whether your marketing is making money. And when it becomes the primary success metric, it actively incentivizes the wrong optimizations: broader targeting, lower-friction offers, higher-volume lower-intent campaigns. All of which look like improvement on paper while quietly degrading your funnel.
The clinics making the best marketing decisions aren't the ones with the lowest CPL. They're the ones who know what they paid for a patient — and whether that patient returned.
Want to See Your Real Cost Per Patient?
Your agency can show you what you paid for a lead. ClinicROI shows you what you paid for a patient.
Connect your ad spend to your booking data and EMR revenue — and see the number your agency report never shows you.
Related articles: